
Study examines characteristics, features of West Nile virus outbreaks from Dallas County housing, hospital and weather data

Book a live interview

To book a live or taped interview with Dr. Thomas Fomby in the SMU News Broadcast Studio call SMU News at 214-768-7650 or email SMU News at news@smu.edu. |
Related Links
- SMU Magazine: Alumnus-Faculty Collaboration Yields Game-changing West Nile Research
- Thomas B. Fomby
- Robert W. Haley
- SMU Department of Economics
- Dedman College
More SMU Research news
 Sweden, SMU psychologists partner to launch parenting program that reduces child abuse
Sweden, SMU psychologists partner to launch parenting program that reduces child abuse Chemical probe confirms that body makes its own rotten egg gas, H2S, to benefit health
Chemical probe confirms that body makes its own rotten egg gas, H2S, to benefit health Study: High-volume Bitcoin exchanges less likely to fail, but more likely to suffer breach
Study: High-volume Bitcoin exchanges less likely to fail, but more likely to suffer breach Musicians who learn a new melody demonstrate enhanced skill after a night’s sleep
Musicians who learn a new melody demonstrate enhanced skill after a night’s sleep Study finds that newlyweds who are satisfied with marriage are more likely to gain weight
Study finds that newlyweds who are satisfied with marriage are more likely to gain weight Fruit flies fed organic diets are healthier than flies fed nonorganic diets, study finds
Fruit flies fed organic diets are healthier than flies fed nonorganic diets, study finds Center for Creative Leadership to study innovative learning method of SMU Lyle School of Engineering
Center for Creative Leadership to study innovative learning method of SMU Lyle School of Engineering NOvA neutrino detector in Minnesota records first 3-D particle tracks in search to understand universe
NOvA neutrino detector in Minnesota records first 3-D particle tracks in search to understand universe Parenting program tackles child abuse and neglect among formerly homeless families
Parenting program tackles child abuse and neglect among formerly homeless families Hiding in plain sight: How invisibility saved New Mexico’s Jicarilla Apache
Hiding in plain sight: How invisibility saved New Mexico’s Jicarilla Apache Study: Most Texas ISDs that are teaching the Bible are skirting 2007 state law
Study: Most Texas ISDs that are teaching the Bible are skirting 2007 state law Study finds Jurassic ecosystems were similar to modern: Animals flourish among lush plants
Study finds Jurassic ecosystems were similar to modern: Animals flourish among lush plants SMU contributes fossils, expertise to new Perot Museum in ongoing scientific collaboration
SMU contributes fossils, expertise to new Perot Museum in ongoing scientific collaboration 100 million-year-old coelacanth discovered in Texas is new fish species from Cretaceous
100 million-year-old coelacanth discovered in Texas is new fish species from Cretaceous Academic achievement improved among students active in structured after-school programs
Academic achievement improved among students active in structured after-school programs Texas frontier scientists who uncovered state’s fossil history had role in epic Bone Wars
Texas frontier scientists who uncovered state’s fossil history had role in epic Bone Wars Observed! SMU’s LHC physicists confirm new particle; Higgs ‘God particle’ opens new frontier of exploration
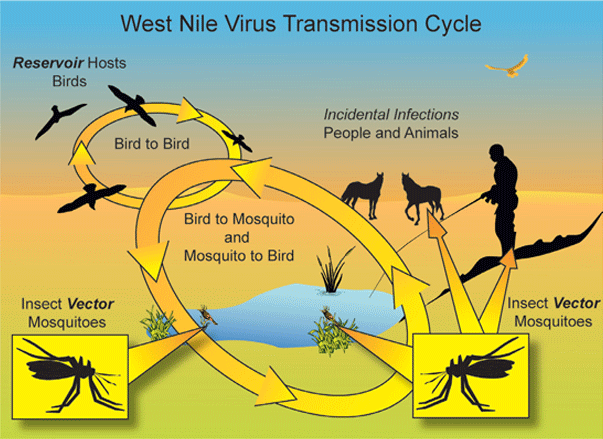
Observed! SMU’s LHC physicists confirm new particle; Higgs ‘God particle’ opens new frontier of explorationResearchers who analyzed a decade of data related to West Nile Virus and, in particular, the 2012 West Nile epidemic in Dallas County, have identified important precursors of West Nile Virus outbreaks that allow for early and effective intervention.
An analysis of the West Nile data, along with weather and housing data, found that the epidemics begin early, after unusually warm winters; are often in similar geographical locations; and are predicted by an index based on an estimate of the average number of West Nile virus-infected mosquitoes collected per trap-night, called the Mosquito Vector Index.
As a result of their data analysis, the researchers recommend the use of a vector-index rating system to identify the best timing and location of early interventions.
The researchers, from Southern Methodist University, UT Southwestern Medical Center and Dallas County Health and Human Services, reported the findings in the July 17 issue of The Journal of the American Medical Association.
The analysis revealed a mosquito vector index rating of 0.5 in June or July as the best time to act to avoid an outbreak and stave off the resultant rise in human West Nile infections, which can cause long-term neurological damage and even death.
“In years when the vector index didn’t start up until late July or August, impending outbreaks just sputtered — in late summer mosquito abundance declines and mosquitoes become less active and stop biting as much. When the vector index goes above .5 early — June or July — right then large numbers of people are silently getting infected, and this should be the best time to intervene,” said senior author Robert W. Haley, Chief of Epidemiology and Professor of Internal Medicine at UT Southwestern.
“After the infecting mosquito bite, on average it takes a week for the first symptoms to develop, a week to see people turning up at hospitals, and a week for laboratory confirmation of the diagnosis and reporting to health officials,” Haley said. “That three weeks is critical. Acting early from the vector index rather than after human case reports and deaths mount up can nip an outbreak in the bud. However, if mosquito data are unavailable or consensus to intervene takes longer, later intervention may still be important to terminate the outbreak.”
The analysis found also that less of a hard freeze during winter months and unusually warm spring temperatures contributed to epidemic years for West Nile, a major concern as global temperatures continue to warm, Haley said.
A fourth critical finding in the paper related census track data to the 2012 outbreak, showing that areas of higher property values, higher housing density, and higher percentages of unoccupied homes were at higher risk. That’s likely due to fostering the types of environment and mosquitos most likely to transmit the disease, which is carried more by house mosquitoes than wooded mosquitoes. In Dallas County, the data showed year-after-year clustering in the Park Cities and North Dallas areas.
Study authors supply instruction manual for other counties
The analysis tools used in the study may be applicable elsewhere, but due to variations in weather, mosquito populations and other factors, each region or county will need to conduct its own analysis to identify the most appropriate vector index rating signaling when to act, Haley said. Along with the paper, the authors provide an instruction manual for other counties to calculate the vector index from their own mosquito infection surveillance data.
“Given the leading character of this index, epidemiologists and government officials can implement, in a more timely manner, preventative measures to reduce the impact of future West Nile Virus outbreaks,” said data modeling expert Thomas B. Fomby, Professor of Economics and the Director of the Richard B. Johnson Center for Economic Studies at SMU.
Fomby provided the time series expertise needed to analyze the leading nature of the vector index and determine that aerial spraying used during the epidemic did not have any significant adverse health effects on the general public.
“Time Series Count modeling and Event Analysis are statistical methods that are frequently used in economic research but not so often used in medical research,” Fomby said. “Time Series Count modeling was used to investigate the leading nature of the vector index while Event Analysis was used to examine the impacts of aerial spraying. This is a prime example of where interdisciplinary tools can be useful in conducting scientific research.”
Other authors of the study were physician Wendy Chung, Chief Epidemiologist, and her associates Christen Buseman, Sibeso Joyner and Sonya Hughes, all of Dallas County Health and Human Services; and James Luby, professor of internal medicine in the Division of Infectious Diseases at UT Southwestern.
West Nile virus first identified in Dallas County in 2002
“After declining over the prior 5 years, mosquito-borne West Nile virus infection resurged in 2012 throughout the United States, most substantially in Dallas County, Texas. Dallas has been a known focus of mosquito-borne encephalitis since 1966, when a large epidemic of St. Louis encephalitis (SLE) occurred there, necessitating aerial spraying of insecticide for control,” according to background information in the article.
“With the introduction of West Nile virus into New York City in 1999 and its subsequent spread across the country, West Nile virus appears to have displaced SLE virus,” the authors wrote. “Dallas recognized its initial cases of West Nile virus encephalitis in 2002 and its first sizeable outbreak in 2006, followed by 5 years of low West Nile virus activity. In the 2012 nationwide West Nile virus resurgence, Dallas County experienced the most West Nile virus infections of any U.S. urban area, requiring intensified ground and aerial spraying of insecticides.”
Study analyzed multitude of data, from infections to weather to geography
The study examined the features associated with the West Nile virus epidemics to identify surveillance and control measures for minimizing future outbreaks.
The researchers analyzed surveillance data from Dallas County (population, 2.4 million), which included the numbers of residents diagnosed with West Nile virus infection between May 30, 2012 and Dec. 3, 2012; mosquito trap results; weather data; and syndromic (pertaining to symptoms and syndromes) surveillance from area emergency departments.
From May 30 through Dec. 3, 2012, patients with any West Nile virus-positive test result were reported to the health department; 615 met laboratory case criteria, and 398 cases of West Nile virus illness with 19 deaths were confirmed by clinical review in residents of Dallas County.
The outbreak included 173 patients with West Nile neuroinvasive disease (WNND) and 225 with West Nile fever, and 17 West Nile virus-positive blood donors. Regarding patients with WNND, 96 percent were hospitalized; 35 percent required intensive care; 18 percent required assisted ventilation; and the case-fatality rate was 10 percent. The overall WNND incidence rate in Dallas County was 7.30 per 100,000 residents in 20l2, compared with 2.91 in 2006.
The first West Nile virus-positive mosquito pool of 2012 was detected in late May, earlier than in typical seasons. Symptoms of the first 19 cases of WNND in 2012 began in June, a month earlier than in most prior seasons; thereafter, the number of new cases escalated rapidly. Sequential increases in the weekly vector index early in the 2012 season significantly predicted the number of patients with onset of symptoms of WNND in the subsequent l to 2 weeks.
West Nile neuroinvasive disease clustered in neighborhoods with high housing density
The 2012 epidemic year was distinguished from the preceding 10 years by the mildest winter, as indicated by absence of hard winter freezes, the most degree-days above daily normal temperature during the winter and spring and other features. During the 11 years since West Nile virus was first identified in Dallas, the researchers found that the annual prevalence of WNND was inversely associated with the number of days with low temperatures below 28 degrees Fahrenheit in December through February.
“Although initially widely distributed, WNND cases soon clustered in neighborhoods with high housing density in the north central area of the county, reflecting higher vector indices and following geospatial patterns of West Nile virus in prior years,” the authors write.
Aerial insecticide spraying was not associated with increases in emergency department visits for respiratory symptoms or skin rash.
“This report identifies several distinguishing features of a large urban West Nile virus outbreak that may assist future prevention and control efforts for vector-borne infections,” the authors write. “Consideration of weather patterns and historical geographical hot spots and acting on the vector index may help prevent West Nile virus-associated illness.” — UT Southwestern, JAMA, SMU
Follow SMUResearch.com on Twitter.
For more information, www.smuresearch.com.
SMU is a nationally ranked private university in Dallas founded 100 years ago. Today, SMU enrolls nearly 11,000 students who benefit from the academic opportunities and international reach of seven degree-granting schools. For more information see www.smu.edu.
SMU has an uplink facility located on campus for live TV, radio, or online interviews. To speak with an SMU expert or book an SMU guest in the studio, call SMU News & Communications at 214-768-7650.